Coronavirus isn’t killing Oregon’s economy, the lockdown is
By Professor Hinkley April 17, 2020

more harm than good?
This morning, a group of Stanford researchers released their much-anticipated data on the prevalence of SARS-CoV-2 antibodies in Santa Clara County. The researchers noted that their data “implies that the infection is much more widespread than indicated by the number of confirmed cases.”
As they further explained, “population prevalence estimates can now be used to calibrate epidemic and mortality projections.”
It’s that second quote that really matters, but I’m not sure you’re going to like what the data tells us, at least if you’re someone who thinks the choice to lockdown—and continue to lockdown—our beautiful state by Governor Kate Brown was a prudent decision. Here’s what we now know about the difference between confirmed positive tests in the general population, and the actual number of people who have been infected with COVID-19:
“These prevalence estimates represent a range between 48,000 and 81,000 people infected in Santa Clara County by early April, 50-85-fold more than the number of confirmed cases.”
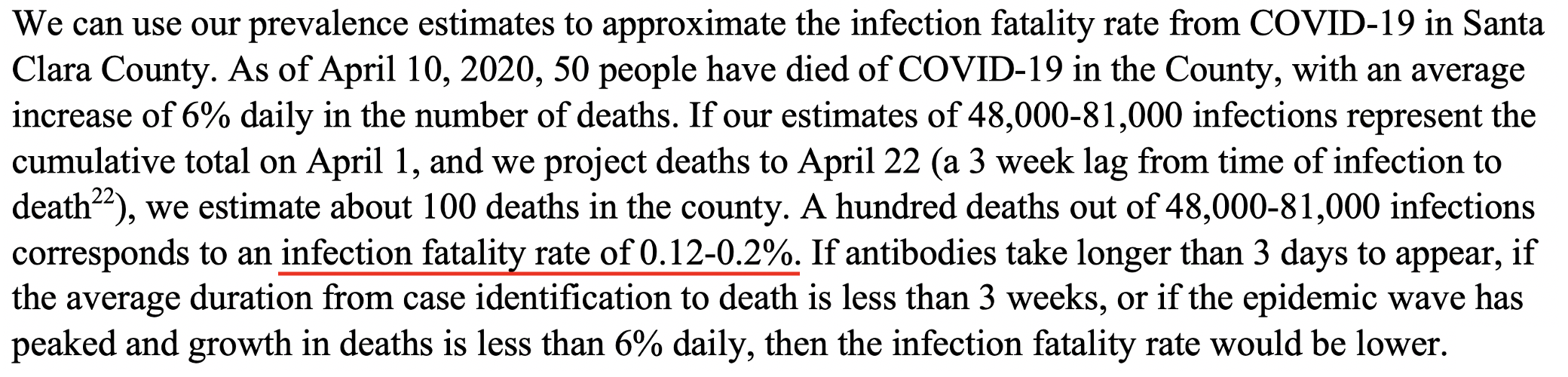
Simple enough, right? There are somewhere between 50-85x more people infected by COVID-19 than those who actually have tested positive for it. The ranges are still pretty broad, because we’re in the early days, but even this broad range can help us quite a bit in determining a number that really matters: COVID-19’s mortality rate in the general population. And what is that rate? Brace yourself. I’ll just share this screenshot from the actual study text:
Click image to see paper
If you’ve been paying close attention to this topic, you already realize how seismic the data coming out of Stanford really is. We just shut down our economy, we are incurring unknown and incalculable destruction—including death—from this catastrophic policy decision…for a virus with a fatality rate of 0.12-0.2% and, according to the Stanford researchers, that rate is likely to “be lower.” If you’d like to know where COVID-19 now fits on the scale of disease fatality rate, here’s a simple table, but I will try to put COVID-19 in proper context:
It’s a bad flu (flu is roughly 0.1% mortality rate), although its uniquely bad for people over the age of 80 with co-morbid conditions, and its a mild flu for people under 50, and pretty much no risk for people under 30, especially children.
Let’s put my summary in some perspective using recent data from Florida:

So, in Florida, 93% of the deaths from COVID-19 have been in people 55 years of age or older, with 83% over the age of 65. This is a unique virus that’s particularly nasty for older people, especially those with co-morbidities, of which obesity has been identified as #1. (While we’re on the state of Florida, an extra point I’d like to make: where's their overwhelming surge? Two weeks ago, doom was predicted for Florida, remember all those images of spring breakers and the criticism of Governor Ron DeSantis? Not only did the predicted disaster never happen, but today Florida announced they are already re-opening beaches. The American Spectator has an excellent article this week on the lack of a disaster in Florida, and the non-coverage of that by the mainstream media. It makes you wonder.)
click image for link
Some of you, understandably, may not be ready to leave the comfort of your basement due to a single study out of Stanford, which is why I think the ongoing math on mortality coming out of Oxford University is so compelling. As Oxford scientists explain: “This page is updated daily as new information emerges. It sets out the current Case Fatality Rate (CFR) estimates, the country-specific issues affecting the CFR, and provides a current best estimate of the CFR, and more importantly, the Infection Fatality Rate (IFR).” If you love data, this is the site for you, but I’ll just cut to the chase of their current conclusion:
“Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR somewhere between 0.1% and 0.36%.”
So, not only are the Oxford scientists finding a mortality rate for COVID-19 in line with what Stanford researchers just found (through an entirely different method), but the Oxford researchers also state something that I think is worth mentioning during this time of panic:
“Evaluating CFR during a pandemic is, however, a very hazardous exercise, and high-end estimates should be treated with caution as the H1N1 pandemic highlights that original estimates were out by a factor greater than 10…In Swine flu, the IFR ended up as 0.02%, fivefold less than the lowest estimate during the outbreak.”
What do those words do for me? I’m comforted that the likelihood that COVID-19’s mortality rate is on line with the seasonal flu is very, very high. (Of course, knowing that would mean that all these decisions to lockdown society were unnecessary.)
Is this going to be an annual thing?
Back to the use of a lockdown for a virus with COVID-19’s mortality rate. I have a simple question for you:
How many times do you think Oregon, and the rest of our country, can afford to do a lockdown of this magnitude in our lifetime?
One more time? Two? Three? Don’t new viruses emerge every few years? SARS? MERS? Zika? All the unknown names still to come? Is this our new pandemic strategy? I think you know the answer. We really can’t afford to do this again even once more without bankrupting our state, our country, and all of our small and medium sized businesses. It’s simply an untenable, and unrepeatable, strategy. If you even agree with most of this point, then how high should the standard be for making such a draconian decision, and how solid do the facts need to be to keep it going, to remain under lockdown?
Oregon is now tethered to California, and to “SCIENCE”
I thought I was done writing about COVID-19 and our wasteful lockdown here in Oregon, with posts written on both April 4th and April 8th that argued that we were already on the back side of the epidemic curve of COVID-19 making a lockdown irrational and wasteful, but then California’s Governor Gavin Newsom had to go and do something that always sends up a red flag for me: he invoked “science.” And not even small caps “science,” he invoked SCIENCE in this tweet from three days ago. See for yourself:
Now, as an Oregonian, I really spend very little time caring about or monitoring what California does, but in this case Governor Newsom’s words really matter to me, because apparently our own Governor Kate Brown has made some sort of pact with both California and Washington to all re-open their economies together, once SCIENCE says they can. The invocation of SCIENCE is always dangerous, and in this case its also painfully ironic, because the thing they used both in California and Oregon and Washington to justify a lockdown in the first place was about the least science-based thing they could have ever used: a catastrophically inaccurate model developed by the soon-to-be infamous IHME at the University of Washington, an organization funded by, you guessed it, Bill Gates. The IHME’s original disease model has proved to be so wildly inaccurate that it would be comical if we weren’t destroying our economy trying to conform to its now completely outdated prognostications of doom. Does that sound like science to you?
The IHME: Doomsday is coming
It’s not an exaggeration to say that the doomsday predictions of the IHME’s Coronavirus model are what caused Governors across the country to shut down their economies. Don’t take my word for it, the National Review’s Andrew McCarthy was very eloquent last week in explaining:
“And mind you, when we observe that the government is relying on the models, we mean reliance for the purpose of making policy, including the policy of completely closing down American businesses and attempting to confine people to their homes because, it is said, no lesser measures will do.”
And how does Mr. McCarthy, a senior fellow at the National Review Institute, think these models have performed?
“To describe as stunning the collapse of a key model the government has used to alarm the nation about the catastrophic threat of the coronavirus would not do this development justice.”
What does the science actually say?
I want to be super clear about something. I don’t blame Governor Kate Brown for locking down Oregon when she did. The pressure was incredible. The information she was presented with basically said, “if you don’t do this, tens of thousands of Oregonians will die and our hospitals can’t handle it.” Not only has that information proven to be entirely false, but I believe we’ve also lost our way on the entire point of the lockdown. The point was to make sure we have enough capacity in our hospitals, nothing more, nothing less. If you think the point is to snuff out COVID-19 or keep people from getting it, that’s simply unrealistic, as any public health official would tell you for a virus that is already in the community. Meanwhile, we are absolutely destroying our economy and the future of so many Oregonians, and the data is clearly telling us that’s a bad, bad policy decision. I don’t blame Kate Brown for initiating the lockdown, I very much blame her for continuing the lockdown given the new information we have, which I will now walk you through, with numbers to keep it simple:
1. The case fatality rate is 0.12-.2% for COVID-19, which means its highly likely to end up in the same range as influenza.
As of today, 70 Oregonians have died from Covid-19 according to the Oregon Health Authority website. All deaths of our fellow Oregonians are tragic, but death happens, and simply MUST be put in context, so let’s do just that, here’s the most recent CDC data I could find on deaths in Oregon in a single year, 2017:
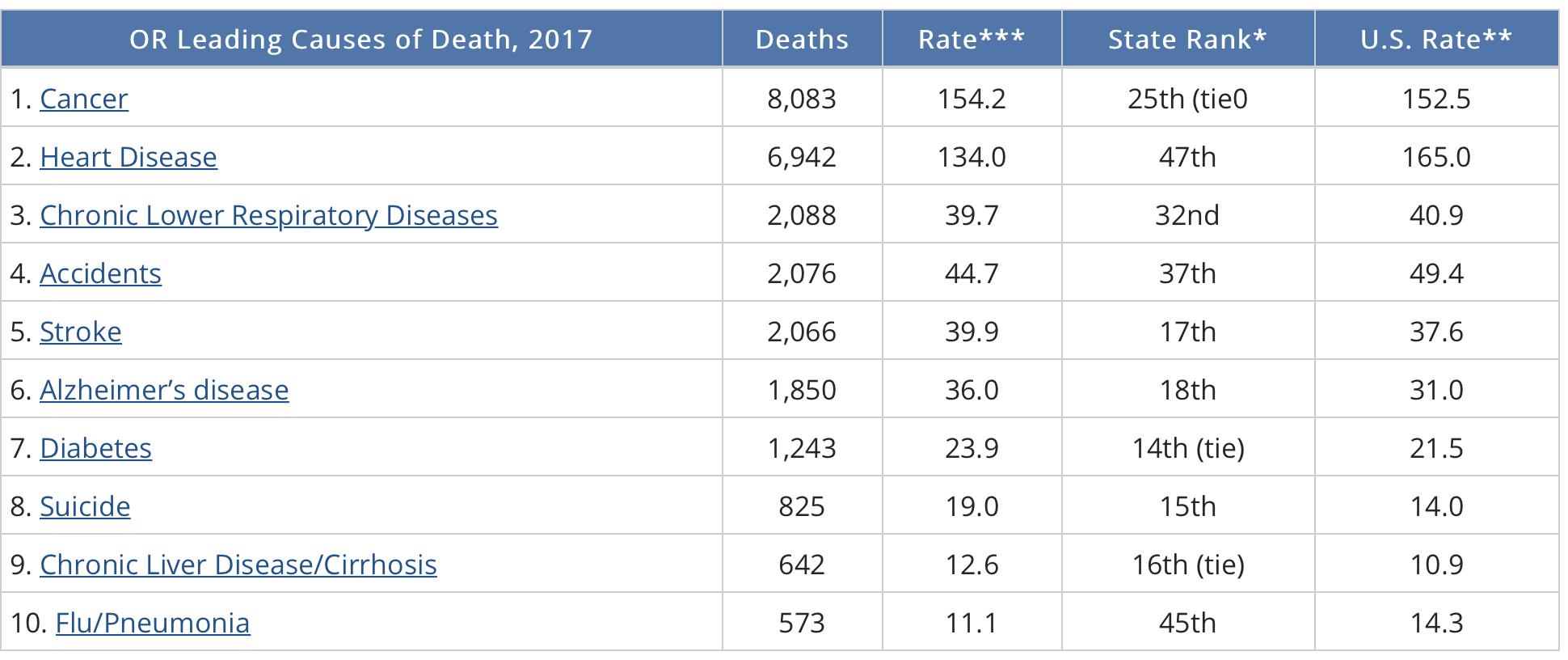
How does this table hit you? When you think about 70 deaths here in Oregon (of which half have been in nursing homes), do you think we should have locked down the state? Do you think we still need to be locked down? Should we do a daily count of every diabetic who dies in Oregon, since we lose almost three every day? If I haven't convinced you yet, please read on.
2. COVID-19 follows the natural bell curve of a virus, and was doing so here in Oregon BEFORE the lockdown took place.
This was the substance of my argument in my post on April 5th, but it’s only more true today. That ALL viruses follow a natural bell curve, with slopes roughly equal on the way up and down, was discovered by Dr. William Farr more than 100 years ago, and it’s known as Farr’s law. Recently, Chinese and American scientists published a study to see if COVID-19 would behave according to Farr’s law, and here’s the chart from their recent paper:
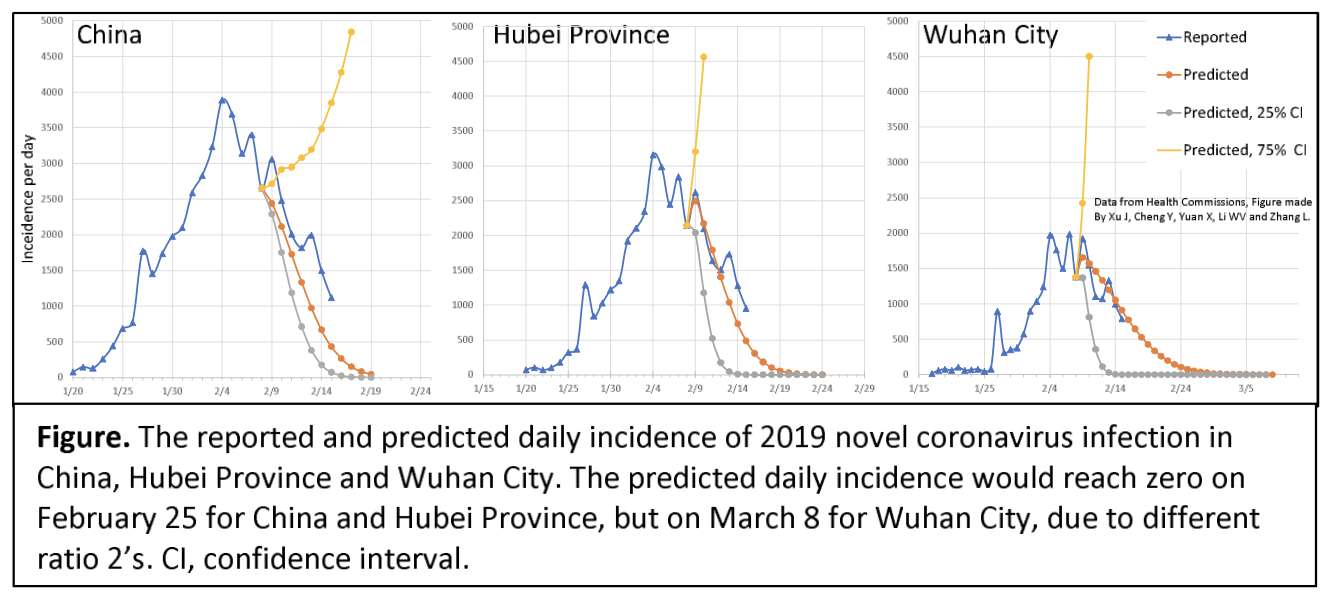
As you can see, the predicted path of the virus in China (orange dotted line) and the actual path of the virus (blue dotted line) are a match. A renowned Israeli scientists recently made this same point, in the middle of Israel’s lockdown:

Dr. Isaac Ben-Israel made the same point I’m trying to make here: viruses follow a predictable pattern, and he made his position to the Israeli public very clear:
A prominent Israeli mathematician, analyst and former general claims simple statistical analysis demonstrates that the spread of COVID-19 peaks after about 40 days and declines to almost zero after 70 days — no matter where it strikes, and no matter what measures governments impose to try to thwart it.
Prof Isaac Ben-Israel, head of the Security Studies program in Tel Aviv University and the chairman of the National Council for Research and Development, told Israel’s Channel 12 (Hebrew) Monday night that research he conducted with a fellow professor, analyzing the growth and decline of new cases in countries around the world, showed repeatedly that “there’s a set pattern” and “the numbers speak for themselves.”
While he said he supports social distancing, the widespread shuttering of economies worldwide constitutes a demonstrable error in light of those statistics. In Israel’s case, he noted, about 140 people normally die every day. To have shuttered much of the economy because of a virus that is killing one or two a day is a radical error that is unnecessarily costing Israel 20% of its GDP, he charged.
You may want to discount what I say, since I’m just some anonymous Oregonian, but go ahead and re-read what Dr. Ben-Israel just told you, and then read his resume for yourself. This guy is big time, and he certainly has more credentials than anyone working at the Oregon Health Authority,
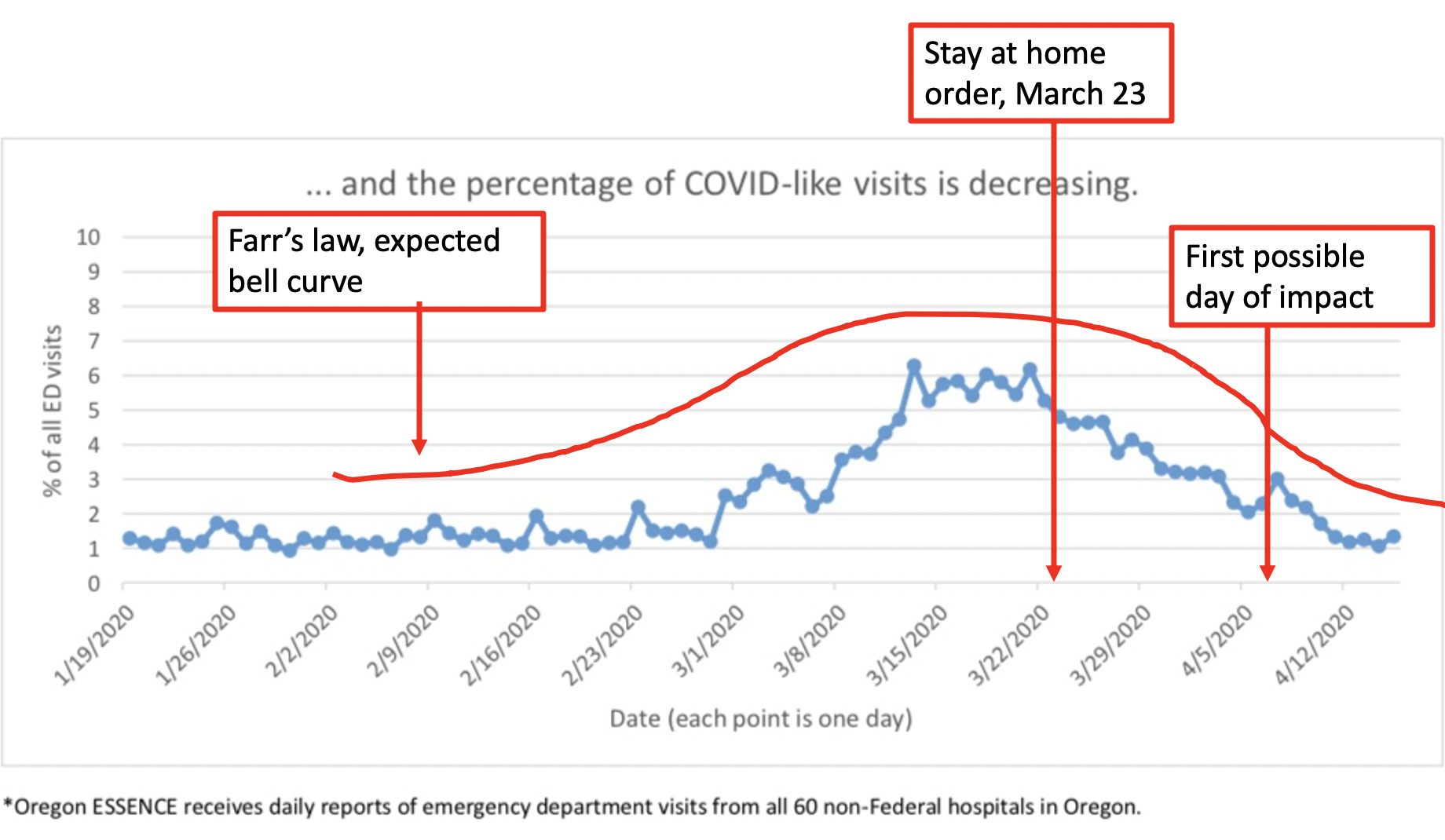
So, let’s look at Oregon’s data right now, according to the OHA, and add in the context of a lockdown to see if Oregon, too, is following Farr’s law, like Dr. Ben-Israel predicts we would and like Chinese and American scientists have already shown was true for China.. Note that, given the time of a lockdown, you shouldn't start to see hospitalizations decline until at least 2 weeks later, based on our understanding of the virus’ timing from exposure to hospitalization.

Do me a favor, re-read Dr. Ben-Israel’s words above, look at Oregon’s data, and then answer honestly: do you really think the lockdown has had any bearing on the outcome here? Not convinced yet? Let’s look at Oregon’s data again from a different perspective—the percentage of emergency room visits, by day, where the patient exhibited possible symptoms of COVID-19—also from today’s OHA report:
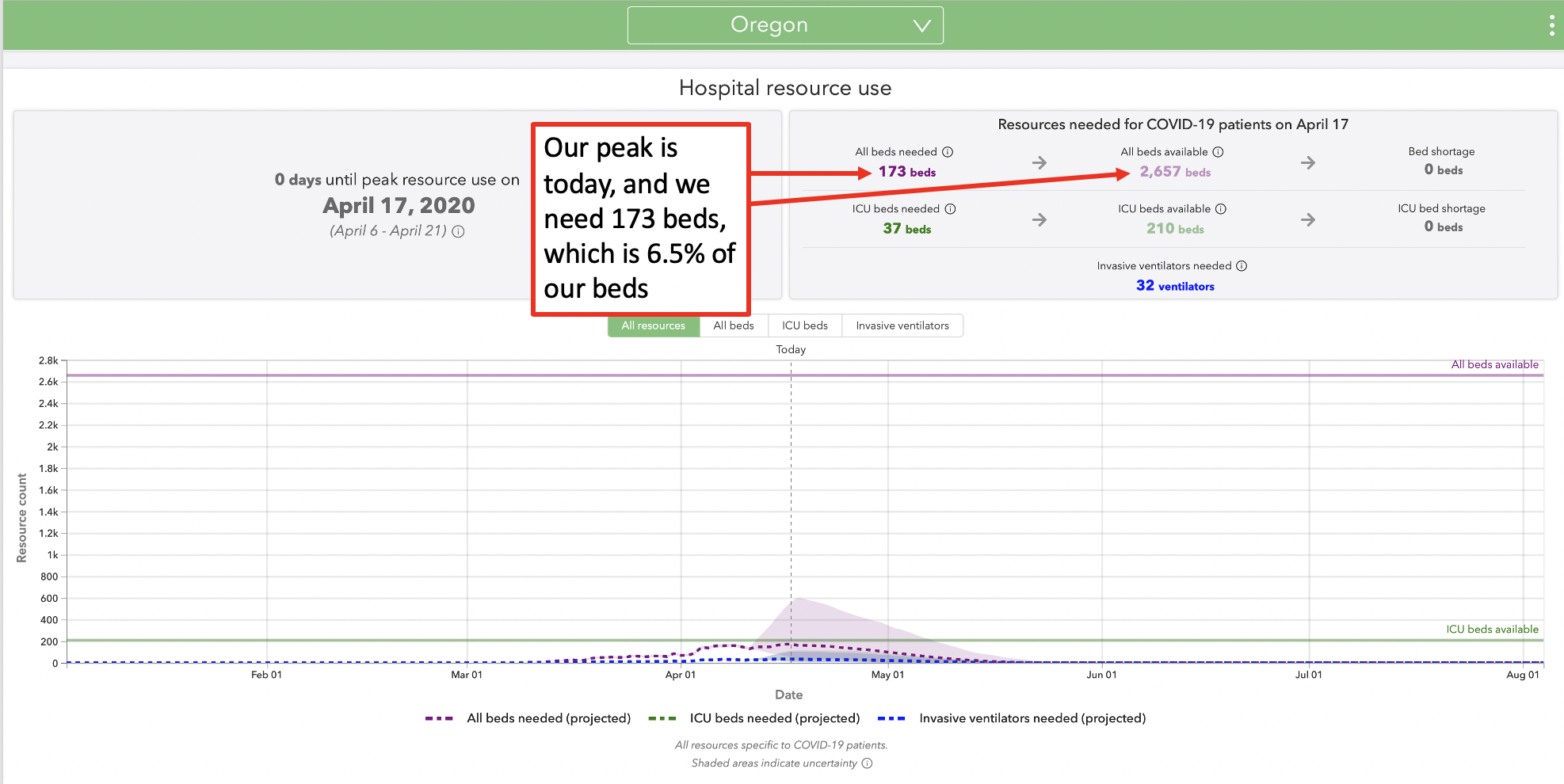
3. The purpose of the lockdown was to ensure Oregon would have enough hospital beds to manage COVID-19 patients. We have zero risk.
I will refer to the current model by the IHME, because that was not only the IHME model’s purpose but has always been the SOLE purpose of a lockdown: to ensure that patients with COVID-19 infections receive proper medical care. What does the model say today? It says we only need 6.5% of total beds in Oregon for COVID-19, and that TODAY is our peak day of use…so why in the hell are we still locked down? We won, we did it! Our hospitals are not strained, now can I please go sit in my favorite coffee shop? (On a sad note, hospitals all over the country are actually getting wiped out financially, because they all canceled elective procedures awaiting a surge that never came. Read for yourself.)
I want to make a special point: please challenge circular reasoning. People will read this and say, “well the reason we haven’t taxed our hospital resources here in Oregon is because we locked down and flattened the curve.” That’s simply not true, which is what I explained in Point #2 above. The virus was going to do what it was going to do, which is largely because the virus has been here in circulation much longer than people thought, and any lockdown happened way too late in it’s natural cycle. You can prove that with the bell curve here inOregon, and with the fact that the Stanford researchers found way more people infected. The lockdown was late, and useless. It’s only caused economic harm. And, by the way, the IHME model that predicted such draconian outcomes and scare so many Governors into lockdowns did so while ASSUMING LOCKDOWNS were in place. I really enjoyed this post talking about how COVID-19 has been in the U.S. since November, check it out.)
4. According to the science, social distancing and shutting down stores has little bearing on the spread of the virus, but it is ruining our economy and many people’s lives and livelihood
Professor Hendrik Streeck from the University of Bonn is leading a study in Germany on the hard-hit region of Heinsberg and his conclusions, from laboratory work already completed, will probably infuriate you:

click image to read article
Streeck and his team are attempting to root out the sources of infection by studying residents of the northwestern region. Speaking to press on Tuesday, he said most cases of coronavirus in Heinsberg originated from people being close together for a significant period of time, and not from touching surfaces with virus particles on them…
Streeck went on to say that though the virus could "live" on various surfaces for up to seven days, he believed there was little chance that someone could become infected via surfaces…
Instead, claims Streeck, his study found that: "There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time.“When we took samples from door handles, phones or toilets it has not been possible to cultivate the virus in the laboratory on the basis of these swabs….”
Uh oh. You mean closing parks, closing stores, wearing gloves at the grocery store, fumigating our groceries, and just being generally paranoid wasn't necessary? As Dr. Streeck confirms:
"It is important to obtain this data in order to make sure that decisions are taken based on facts rather than assumptions. The data should serve as a basis of information for the government so they can then think about their further course of action," he said.
And he continues:
“People could lose their jobs. They might not be able to pay their rent anymore and staying inside for a longer time can lead to weakening of our immune system.” He raises questions like: “The goal is not a complete containment of the virus. We need to know where the actual capacity limits of our hospitals are. How many infections are too many? What do intensive care medics say?”
“It is important to start thinking about a “rollback” strategy and his hope is to “deliver the relevant facts so that people have a good foundation for their decisions.”
Not convinced by Dr. Streeck’s preliminary conclusions from his study in Germany? Still think everyone needs to be wearing a mask and gloves at the grocery store? Well, published science from China showed exactly the same thing. In a study titled, Indoor transmission of SARS-CoV-2, scientists studied outbreaks of 3 or more people in 320 separate towns in China over a five-week period beginning in January 2020 trying to determine WHERE outbreaks started: in the home, workplace, outside, etc.? What’d they discover? Almost 80% of outbreaks happened in the home environment. The rest happened in crowded buses and trains. But what about outdoors? I mean, surely Kate Brown must know something since she’s closed all of our parks and beaches, right? The scientists wrote:
“All identified outbreaks of three or more cases occurred in an indoor environment, which confirms that sharing indoor space is a major SARS-CoV-2 infection risk.”
Said differently, there’s really no science to support all the outdoor bans that Oregon, and many other states have put in place, but there is plenty of science to support the fact that sending people home to get cooped up with their family guarantees transmission, which is exactly what happened in Italy. By closing schools and sending everyone home, Italy’s elderly population had their risk of exposure heightened:
Multi-generational households like Ms. Marcone’s are much more common in Italy than in other Western countries. In Italy, around 23% of between the ages of 30 and 49 live with their parents, compared to just 6.4% in the U.S., 5.2% in the U.K or 1% in neighboring France, according to data compiled by the University of Bonn.
5. Closing schools has likely provided little benefit, and done considerable harm, according to recent published science
An article on April 8th in The Lancet tackled the thorny issue of school closures during COVID-19, and has been misinterpreted by many. Frankly, this article is a real breath of fresh air because it takes all these draconian moves being made by state governments and actually PUTS THEM IN CONTEXT of society rather than just narrowly looking at one virus. Here’s one of my favorite passages:

click to read article
Let me pull this important quote out so we can all consider it:
“With over 90% of the world's students (more than 1·5 billion young people) currently out of education, it's clear that the greatest threats from COVID-19 to children and adolescents lie outside the clinic.”
Sweden, an outlier compared with other Western nations, has kept school in session for both primary and junior high school, and here’s why:
“Although universities and sixth-form colleges have closed their physical doors, primary and junior schools have been kept open. Why? Because, says Carlson [Sweden’s head of public health], many children do not have it easy at home. Completing compulsory school is the most important factor in determining their future health.”
By the way, Sweden was predicted to pay a huge price for not shutting their whole country down—you can still go to a restaurant in Sweden—and that hasn’t happened, either. In fact, they, too have a perfect bell curve forming around death from COVID-19, over roughly the same timeframe as all the countries that did lockdown. Sweden will likely be serving as the “control group” for decades to come as we absorb the calamitous decision by so many to shut down:
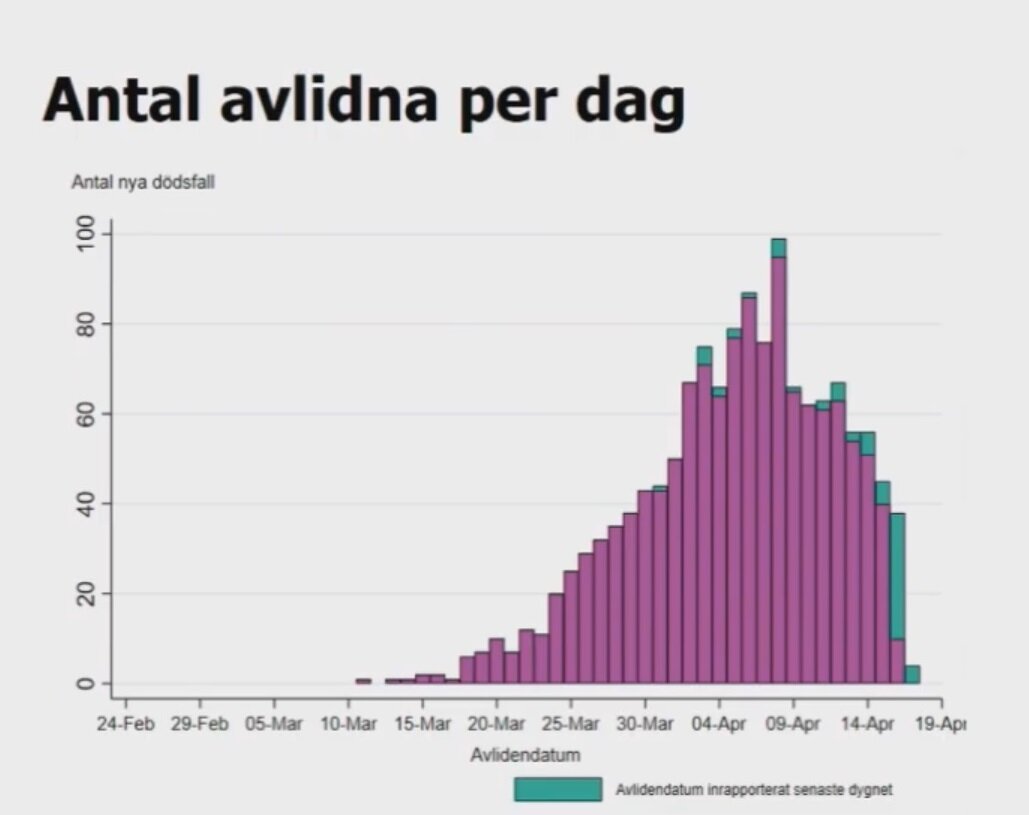
Sweden, deaths per day from COVID-19, click image for source
Finally, to put it back into local context with the information we now have: we shut down all of Oregon’s schools for a disease that doesn’t cause mortality amongst the young, and has an overall mortality rate of 0.12-0.2%, according to Stanford scientists. Yikes.
6. Much greater harm to Oregon will come from unemployment, recession, and economic calamity
As an economics major with years of experience studying infectious diseases, for me this is probably the most frustrating part of the decision-making process Governor Brown and others went through: mortality risk from economic calamity was simply NOT CONSIDERED at all in making the lockdown decision. It wasn't in the IHME model, it’s not in the press, it’s nowhere. And, yet, the science on this topic is readily available and striking, I will just give one quick example from probably the world’s most famous economist on this topic, Dr. M. Harvey Brenner of both Yale and Johns Hopkins. Consider a recent report he provided to the European Union:
In the largest study of its kind on mortality patterns in Europe and the United States, a Yale researcher has found a direct correlation between unemployment and mortality.
The study showed that high unemployment rates increase mortality and low unemployment decreases mortality and increases the sense of well being in a community. Findings from the three-year study, commissioned by the European Union, will be presented to select members of the European Parliament and senior officials at a European Commission press conference on May 23 in Brussels.
“Economic growth is the single most important factor relating to length of life,” said principal investigator M. Harvey Brenner, visiting professor in the Global Health Division of the Department of Epidemiology and Public Health at Yale School of Medicine. Brenner is also professor of health policy and management at Johns Hopkins University and senior professor of epidemiology at Berlin University of Technology.
“Employment is the essential element of social status and it establishes a person as a contributing member of society and also has very important implications for self-esteem,” said Brenner. “When that is taken away, people become susceptible to depression, cardiovascular disease, AIDS and many other illnesses that increase mortality.”
I’ll repeat what he said: “Economic growth is the single most important factor relating to length of life.”
Why have we lost our minds, and any semblance of context?
Death happens. In fact, it’s inevitable for all of us. According to the CDC, 573 Oregonians lost their lives to “Flu/Pneumonia” in 2017. In the same year, 825 Oregonians committed suicide, and cancer took more than 8,000 people. Repealing the national speed limit of 55 has cost us more than 12,000 lives. Should we all wear helmets while driving? Has the world gone crazy? Why can’t we talk about the science that shows all these things are unnecessary? Reminder, 70 people have died in Oregon from COVID-19, and half of those people were in nursing homes.

Says who?
I spent most of today outside here in Portland, it was a beautiful 73 degrees. I saw a young driver, in his own car by himself, wearing a surgical mask. A young family of 5 were out for a bike ride, everyone wearing a mask AND surgical gloves. I hit my favorite grocery store and saw a sign telling me to stand on a bubble to keep everyone safe.
At this point, you probably won’t be too surprised to discover that the 6-foot distance is, in fact, not based on any published science. As this wonderful article explains:
And the commonly held fear that a random passerby will infect a stranger? Here’s more grade-school level talk from the CDC: “COVID-19 is thought to spread mainly through close contact from person-to-person in respiratory droplets from someone who is infected. People who are infected often have symptoms of illness. Some people without symptoms may be able to spread the virus.”
Not only would that sort of conclusion warrant a failing grade in any post-doctoral program, I am pretty sure the average eighth-grade science teacher would take a big red pen to that passage. “Thought.” “Some?” “May?” Keep in mind, there are no links to any scientific studies or papers for the average thinking person to review to decide whether those claims are legitimate.
The CDC also can’t quite make up its mind about the safety of large gatherings in the COVID-era. In mid-March, the agency asked Americans to limit gatherings of 250 people or more. A few weeks later, the White House, at the behest of the CDC, urged Americans to avoid gatherings of more than 10 people. There is no science, however, to support either number. (What is so fateful about 250 people? Why not 175? And why 10 people? Why not 16 or 17?)
The article takes dead aim at so many Governors who are absolutely running with these completely unsupportable recommendations:
Even that fuzzy advice has been bastardized by the petty tyrant lurking inside every big state governor, small-town mayor, and homeowners’ association president. Over the weekend, Michigan Governor Gretchen Whitmer banned people from going to a neighbor’s house. “All public and private gatherings of any size are prohibited,” Whitmer announced. “People can still leave the house for outdoor activities . . . recreational activities are still permitted as long as they’re taking place outside of six feet from anyone else.”…There will be plenty of soul-searching after this crisis abates: demanding to know the scientific rationale for keeping us six feet apart when people needed each other most should be at the top of the list.
Here in Oregon, Governor Brown has even usurped one of our favorite mottos—”Keep Portland Weird”—and bastardized it with the help of Wieden+Kennedy to promote even more hysteria (seriously, this billboard is all over town):

Now what?
I’m going to repeat myself a little bit. I understand Governor Kate Brown’s original decision to shut down Portland’s schools and most businesses. She was being provided with apparently credible information from the IHME that claimed that not only were thousands of Oregonian’s lives at stake, but also our hospitals would be completely overrun if we didn't lockdown.
Some people will make the argument that the act of shutting down is WHY we are in such good shape today, but the bell curve of COVID-19 in Oregon refutes that argument, not to mention what’s happening both in Florida, Sweden and many other places that either never shutdown or shutdown much, much later. (Florida did not shut down until April 3rd. Yet, magically, on their peak day of April 11th, they only needed 1,535 hospital beds out of 20,184 available, just 7.6%—in a state where calamity was predicted not two weeks ago!)
While I agree with Governor Brown’s original decision, the facts are so different today, and honestly there is no reason in the world that Governor Brown shouldn’t immediately:
Open every park and beach
Allow children to return to school
Open all businesses, including retailers and restaurants
Out of an abundance of caution, I do believe special provisions should be made for our most vulnerable, since we have clear, consistent, accurate data that people over 65 with co-morbid conditions have a much higher risk of dying from COVID-19. Nursing homes should, in particular, have an armory of defenses to protect their residents, until a proper treatment is found to reduce mortality. (And, evidence has emerged that early treatment with hydroxychloroquine and azithromycin is likely to be effective in reducing mortality.) Realistically, if you are expecting to keep all of our senior citizens quarantined until a vaccine is ready, you might want to read this interview from a leading vaccine expert. It’s years away, at best, at least according to him.
Unfortunately, we are tethered to the SCIENCE from California’s Governor
As much as I believe there is more than enough scientific evidence to end the lockdown immediately, Governor Brown appears to have cast her lot (and therefore our entire state) with California’s Governor Gavin Newson, agreeing to work in lock-step with whatever he decides. And since he’s the one who said SCIENCE will guide the day (apparently unlike all the science I just shared with you), what exactly does he mean by this? I’ll let him explain what the six “scientific” criteria are to re-open the West Coast:
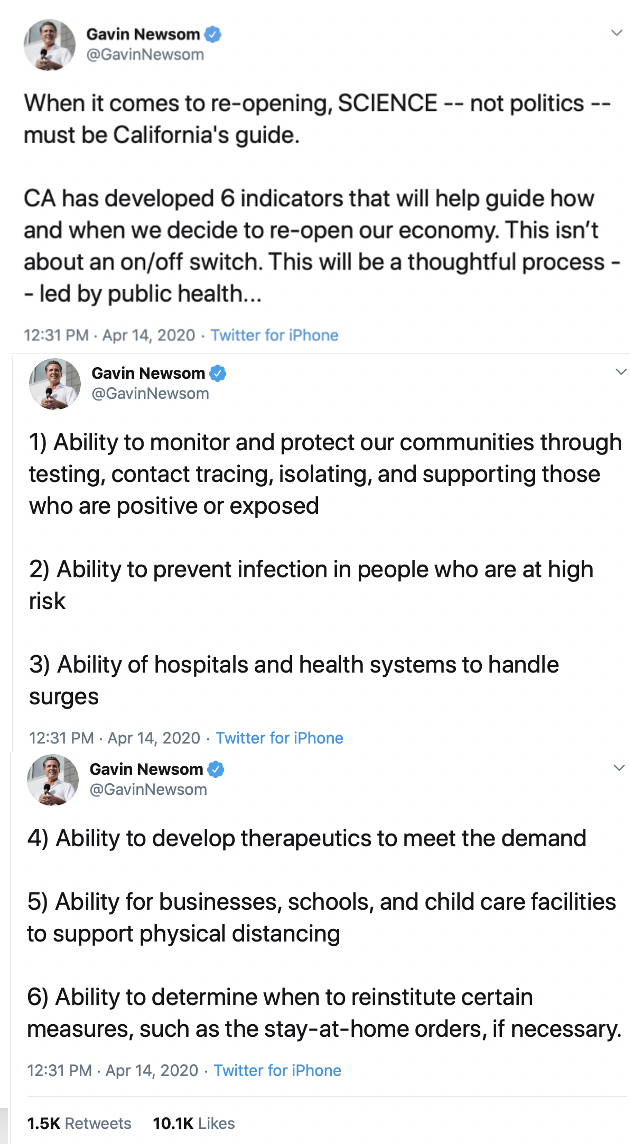
Since these six criteria are apparently the things standing between us and our freedom, I will address them from two perspectives: 1) How do they mesh with the original stated purpose of the lockdowns, which was to take pressure off of our healthcare system, and 2) are they SCIENCE-based criteria?
1) Ability to monitor and protect our communities through testing, contact tracing, isolating, and supporting those who are positive or exposed
This is extremely vague, and lives or dies on the word “ability.” It seems like the right time to bring up an obvious point that no one mentions: California’s peak surge in their hospitals was, according to the model Gover Newsom used, three days ago. Guess how many hospital beds, expressed as a total of beds in California, were used on that peak day? 10.3% That’s it. On March 28th, Governor Newsom said he would need 10,000 ventilators for its peak. How many were in use on the peak day? 550. How can it not already be the case that California (and certainly Oregon) has the “ability” to support those who are “positive or exposed.”
2) Ability to prevent infection in people who are at high risk
I agree that this should be the #1 focus in both Oregon and California. Half of Oregon’s total COVID-19 deaths happened in nursing homes.
3) Ability of hospitals and health systems to handle surges
We are so far past this point that for this to be a criteria is laughable, as explained in Point #1.
4) Ability to develop therapeutics to meet the demand
This has NOTHING to do with why states were locked down in the first place, and holding a state hostage until we’re certain we have the right therapeutics in place makes no sense.
5) Ability for businesses, schools, and child care facilities to support physical distancing
Since the science shows this has very little to do with transmission, this is an unrealistic criteria. And, who exactly monitors and enforces this?
6) Ability to determine when to reinstitute certain measures, such as the stay-at-home orders, if necessary.
For a virus with a mortality rate of 0.12-0.2% from scientists at the leading academic institution in your state, I think the answer here is very clear:
NEVER. As in, NEVER EVER AGAIN.
About Professor Hinkley:
I’m an over-educated Oregonian writing under a pen name because I want to stay employed. I’m sure you understand.

click to read
April 18th Update, Stanford data goes mainstream:
This morning, the Wall Street Journal ran an Op-Ed by Molecular Biologist Andrew Bogan that made many similar points about the implications of the new Stanford study, I liked this passage the best:
“Yet if policy makers were aware from the outset that the Covid-19 death toll would be closer to that of seasonal flu than the millions of American deaths predicted by early models dependent on inputs that now look inaccurate, would they have risked tens of millions of jobs and livelihoods? The science to support better modeling and decision making is rapidly becoming available. One hopes that it will inform better policy decisions.”
April 19th Update, it’s all about Florida:
What’s happening in Florida right now really matters, because it challenges anyone who believes the only reason things aren’t worse is because of the lockdowns. Florida only locked down in early April!! Given the TIME LAG between when someone gets COVID-19 and when they feel bad enough to head to the hospital, we should only now be seeing the impact of a lockdown in Florida, yet the state is already past their peak, and re-opening society! No one can say that Florida’s lockdown has saved them with a straight face, and yet here we are, just look at two headlines (from Fox News and Slate), 2.5 weeks apart.
